Agentic AI in Healthcare: Applications, Benefits, and Challenges
Agentic AI in healthcare goes beyond chatbots and copilots. These autonomous systems plan multi-step clinical workflows, process medical documents, coordinate between hospital systems, and deliver results to clinicians, all while keeping humans in the loop for patient safety. This guide covers what agentic AI actually looks like in practice, where hospitals are deploying it today, and what challenges remain before it scales.

What Agentic AI Means in a Healthcare Context
Most AI tools in healthcare today are reactive. A clinician asks a question, the model answers. A radiologist uploads a scan, the algorithm flags anomalies. These are useful, but they still require a human to initiate every step.
Agentic AI works differently. An agentic system receives a high-level goal, breaks it into subtasks, executes those subtasks across systems, and reports back with results. In healthcare, that might look like an AI agent that monitors new orders in the electronic health record (EHR), determines whether prior authorization is needed, pulls the relevant clinical documentation, submits the request to the payer, and tracks approval status. No one asked it to do each step. It planned and executed the workflow autonomously.
The distinction matters because healthcare runs on multi-step processes that span departments, systems, and organizations. A prior authorization request touches the EHR, clinical documentation, payer portals, and follow-up queues. A clinical trial screening process requires matching patient records against inclusion criteria across dozens of active studies. These are workflows where the overhead isn't in any single step. It's in the coordination between steps.
Agentic AI is purpose-built for that coordination layer. According to a 2026 Deloitte survey, 61% of healthcare organizations are already building agentic AI initiatives or have secured budgets for them, and 85% plan to increase investment over the next two to three years.
That said, only about 3% have deployed agents in live clinical workflows. The gap between interest and deployment is where most of the practical questions live.
Where Hospitals Are Deploying Agentic AI Today
The use cases gaining traction fall into two categories: administrative automation and clinical decision support. Administrative applications are moving faster because the risk profile is lower and the ROI is easier to measure.
Prior authorization automation is the highest-priority use case. According to IDC, 70% of health plans are prioritizing agentic AI for utilization management and prior authorization. The traditional process takes days of back-and-forth between providers and payers. An agentic system compresses that to minutes by collecting clinical documents from the EHR, reviewing payer-specific policies, populating authorization forms, submitting requests, and monitoring status. AWS, UiPath, and startups like Penguin AI and Cohere Health all ship prior authorization agents.
Clinical documentation is the second major category. AI agents listen to patient-provider conversations, generate structured visit notes (SOAP notes, discharge summaries, referral letters), and push them into the EHR for clinician review. The American Medical Association reports that organizations using AI-driven documentation save over 15,000 hours annually.
Patient intake and scheduling agents handle appointment booking, insurance verification, prescription refill requests, and lab result delivery. A California-based health system reported automating routine patient interactions at scale using pre-built healthcare agents, freeing clinical support staff for complex cases.
Adverse event detection is an emerging application. Researchers have trained AI agents to scan patient records, identify adverse events, generate reports, and route them to clinicians and clinical research coordinators. These systems process hundreds of patient notes in minutes instead of the hours or days that manual review requires.
ICU monitoring represents the clinical frontier. Mount Sinai Health System has deployed AI agents in intensive care units that alert nurses to risks like malnutrition, clinical deterioration, and fall risk while filtering out false alarms that contribute to alert fatigue.
The Technical Architecture Behind Healthcare AI Agents
Healthcare agentic AI systems share a common architecture, even though implementations vary. Understanding the building blocks helps evaluate which solutions are production-ready versus which are demos with a press release.
Orchestration layer. Every agentic system needs a coordinator that breaks goals into subtasks, assigns them to specialized sub-agents, tracks progress, and handles failures. In healthcare, the orchestrator also enforces guardrails: which actions require human approval, which data sources the agent can access, and what happens when confidence drops below a threshold.
Specialized sub-agents. Rather than one monolithic model, most healthcare systems use a team of agents with narrow responsibilities. A prior authorization workflow might include a documentation agent (pulls clinical records), a policy agent (interprets payer requirements), a form agent (fills and submits requests), and a monitoring agent (tracks status and escalates denials). Each agent is optimized for its specific task.
EHR integration. The hardest infrastructure problem. Agents need read access to patient records, clinical notes, lab results, and medication lists, plus write access to update forms, attach documents, and trigger notifications. HL7 FHIR APIs are the standard integration path, but real-world EHR systems often require custom connectors, and data quality varies wildly between installations.
Audit and explainability. Healthcare demands complete traceability. Every agent action, every data access, every decision point needs to be logged with timestamps, reasoning traces, and confidence scores. This isn't optional. It's a regulatory requirement and a clinical safety necessity.
Human-in-the-loop checkpoints. The architecture must define where autonomous execution pauses for human review. High-stakes decisions (medication changes, treatment recommendations, diagnostic conclusions) require clinician sign-off. Lower-risk administrative tasks (appointment scheduling, form submission) can run with post-hoc review.


Give your healthcare AI agents a persistent workspace
50GB free storage with auto-indexing, semantic search, and structured document extraction. No credit card, no trial expiration. Connect agents via the Fast.io MCP server.
How Document Processing Fits Into Clinical AI Workflows
Healthcare generates an enormous volume of documents: clinical notes, insurance forms, lab reports, consent documents, referral letters, imaging reports, discharge summaries. Most of these arrive as PDFs, scanned images, or faxes. Converting them into structured, queryable data is where agentic AI creates the most immediate value.
A document processing agent receives an unstructured file, classifies it (is this a lab report, a prior authorization form, a consent document?), extracts the relevant fields (patient ID, diagnosis codes, dates, provider signatures), validates the extraction against known schemas, and routes the structured data to the appropriate downstream system.
This is different from traditional OCR or template-based extraction. Agentic document processors handle variation. They work across document layouts, handwriting styles, and formatting inconsistencies because they use language models to understand context, not just pattern matching to find text in expected locations.
For teams building healthcare AI workflows, the document processing layer needs a persistent storage and indexing system. Clinical documents need to be stored with versioning, searchable by content, and accessible to both AI agents and human reviewers.
Tools like Fast.io's Metadata Views address this by letting users describe extraction fields in natural language, after which AI designs a typed schema and populates a sortable, filterable spreadsheet from uploaded documents. PDFs, scanned pages, images, and handwritten notes are all supported. For healthcare-adjacent use cases like insurance document processing, claims review, or research paper synthesis, this kind of structured extraction eliminates manual data entry while keeping humans in the review loop.
The broader point: agentic AI in healthcare isn't just about the model's intelligence. It's about the infrastructure for storing, indexing, searching, and handing off documents between agents and clinicians. Intelligence-enabled workspaces that auto-index files for semantic search and citation-backed chat provide the foundation that clinical AI agents need to operate reliably.
Risks and Challenges That Slow Adoption
The 3% live deployment rate tells you something important: healthcare organizations want agentic AI, but the barriers are real.
Patient safety is non-negotiable. When an agentic system makes an error in an e-commerce recommendation engine, someone sees the wrong product. When it makes an error in a clinical workflow, a patient could receive the wrong treatment. Autonomous systems that execute multi-step processes create the risk of cascading failures, where one incorrect decision propagates through downstream actions before anyone catches it. Building reliable human-in-the-loop checkpoints at the right places in the workflow is the central engineering challenge.
Data bias creates health equity risks. AI agents learn from training data, and healthcare data reflects decades of systemic disparities in treatment, diagnosis, and outcomes across racial, socioeconomic, and geographic lines. An agent trained on biased data will perpetuate those biases at scale, potentially widening health equity gaps instead of closing them.
Security surface area expands dramatically. A single agentic system can touch EHRs, payer portals, scheduling systems, lab databases, and communication platforms. Each integration point is an attack surface. Prompt injection attacks are a specific concern in multi-agent systems: a malicious payload injected into one agent can cascade through the entire chain. Healthcare organizations need defense-in-depth strategies that go beyond perimeter security.
Accountability remains legally unsettled. When an agentic AI system contributes to a clinical error, who is liable? The clinician who approved the workflow? The hospital that deployed the system? The vendor that built the agent? The legal frameworks haven't caught up. The EU's Medical Device Regulation Article 14 mandates human oversight for high-risk AI systems, but enforcement specifics are still emerging.
Interoperability is fragmented. Healthcare runs on a patchwork of EHR systems, billing platforms, lab information systems, and payer portals. Most of these systems were not designed for machine-to-machine communication. FHIR APIs help, but coverage is inconsistent, and many critical workflows still depend on fax machines and manual data entry.
Clinician trust takes time to build. Even when the technology works, adoption depends on clinicians trusting the system enough to integrate it into their workflows. That trust is built through transparency (showing the agent's reasoning), reliability (consistent accuracy over time), and control (easy override mechanisms when the clinician disagrees).
Building Toward Production-Ready Healthcare AI
Organizations moving from pilot to production are converging on a set of practical principles.
Start with administrative workflows. Prior authorization, scheduling, and documentation are lower-risk, higher-volume processes where agentic AI delivers clear ROI without touching clinical decision-making directly. Build organizational confidence and technical infrastructure with these use cases before expanding to clinical applications.
Design for audit from day one. Every agent action should be logged, traceable, and reviewable. This means structured logging with timestamps, decision rationale, confidence scores, data sources accessed, and actions taken. Don't bolt auditing on after deployment. Build it into the agent architecture.
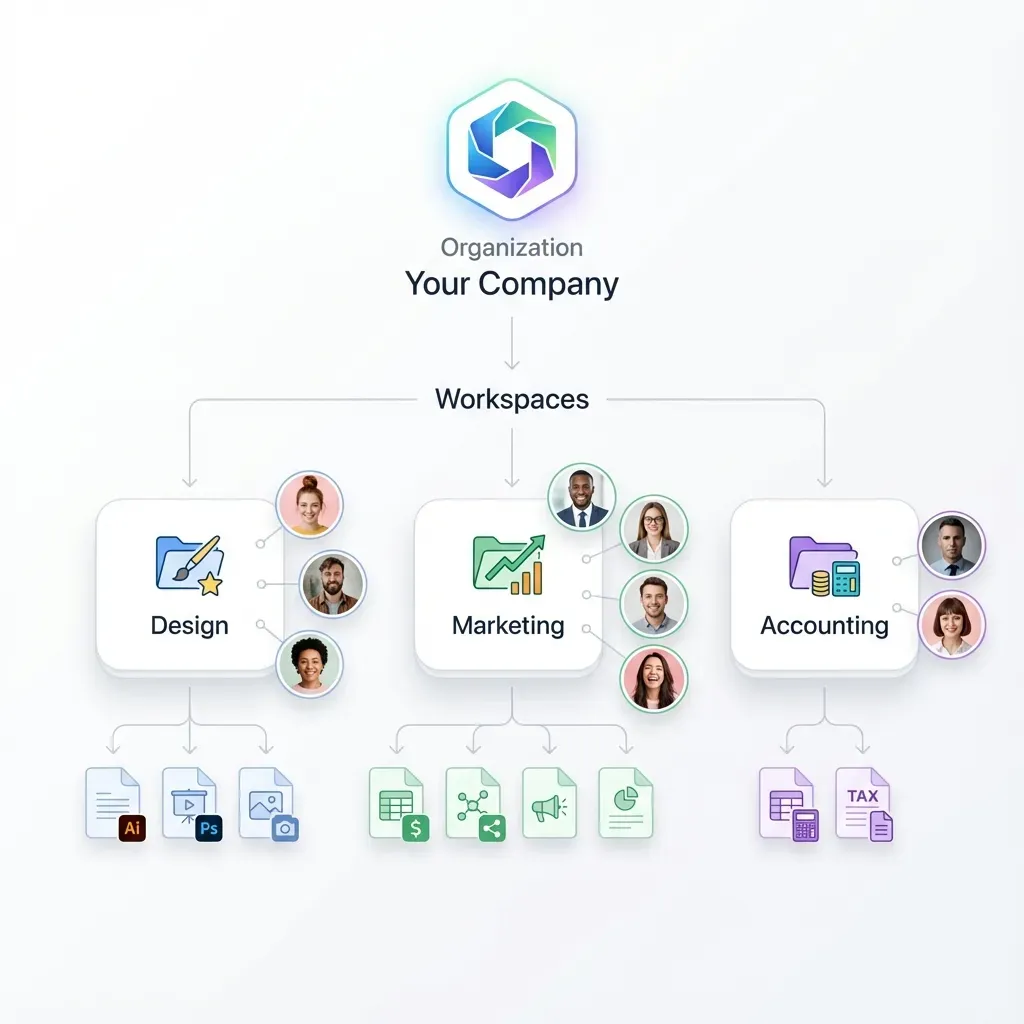
Use workspace-based collaboration. Clinical AI workflows involve handoffs between agents, between agents and clinicians, and between departments. A shared workspace model, where agents and humans operate on the same files, permissions, and audit trails, reduces the coordination overhead that kills complex deployments. Platforms like Fast.io provide this kind of shared workspace with built-in intelligence features, including auto-indexing for semantic search, citation-backed chat, and structured data extraction through Metadata Views.
Implement graduated autonomy. Not every task needs real-time human approval, and not every task should run fully autonomously. Map each workflow step to a risk level, and assign oversight accordingly. Form submission might run autonomously with post-hoc audit. Medication-related recommendations should require clinician sign-off before execution.
Validate continuously, not just at deployment. Healthcare data distributions shift over time. New drug approvals, updated clinical guidelines, changes in payer policies, and seasonal disease patterns all affect how agents should behave. Build monitoring that detects performance degradation and triggers revalidation before errors reach patients.
Plan for the handoff. The most reliable healthcare AI systems are designed around the moment when the agent hands results to a clinician. That handoff needs to include not just the output but the reasoning, the confidence level, the data sources consulted, and a clear mechanism for the clinician to override or modify the agent's work.
Frequently Asked Questions
How is agentic AI used in healthcare?
Agentic AI handles multi-step healthcare workflows autonomously. The most common applications include prior authorization automation, clinical documentation (generating visit notes from patient encounters), patient intake and scheduling, adverse event detection in medical records, and ICU monitoring. These agents plan and execute across multiple systems, like EHRs and payer portals, while keeping clinicians in the loop for safety-critical decisions.
What are examples of AI agents in hospitals?
Mount Sinai uses AI agents in ICUs to monitor patient deterioration and reduce false alarms. Mayo Clinic is piloting VoiceCare AI for back-office automation. Stanford Health Care deploys agents to access personalized real-world evidence. Humana uses AI agents in call centers for member support. Several health systems use documentation agents that listen to patient-provider conversations and generate structured EHR notes.
Is agentic AI safe for healthcare?
Safety depends entirely on implementation. Agentic AI introduces risks that traditional AI tools don't, because autonomous multi-step execution can create cascading errors. Production-ready systems mitigate this with human-in-the-loop checkpoints at high-risk decision points, comprehensive audit trails, graduated autonomy (full automation for low-risk tasks, clinician approval for high-risk ones), and continuous monitoring for performance degradation. The EU's Medical Device Regulation Article 14 mandates human oversight for high-risk AI systems.
What is the difference between AI and agentic AI in healthcare?
Traditional healthcare AI is reactive: a model analyzes input and returns a result (flagging an anomaly on a scan, summarizing a clinical note). Agentic AI is proactive: it receives a goal, plans a multi-step workflow, executes across systems, and reports results. A diagnostic AI reads one image. An agentic system monitors new orders, determines if prior authorization is needed, collects documentation, submits requests, and tracks approvals, all without someone initiating each step.
What is the market size for AI in healthcare?
The healthcare AI market is projected to reach between $110 billion and $194 billion by 2030, depending on the research source and scope definition. MarketsandMarkets estimates $110.61 billion at a 38.6% CAGR. Allied Market Research projects $194.4 billion. Growth is driven by administrative automation, clinical decision support, drug discovery, and the expansion of agentic AI systems that can manage entire workflows autonomously.
How do healthcare organizations handle AI audit trails?
Production healthcare AI systems log every agent action with timestamps, reasoning traces, confidence scores, data sources accessed, and outcomes. This audit trail serves both regulatory compliance and clinical safety. When an agent processes a prior authorization request, for example, the log captures which clinical documents were retrieved, which payer policies were applied, what the submission contained, and whether the request was approved or denied. Clinicians can review the full chain of reasoning for any agent decision.
Can agentic AI reduce healthcare administrative costs?
Early evidence is promising. According to a 2026 Deloitte survey, 98% of healthcare executives expect at least 10% cost savings from agentic AI, with 37% expecting savings above 20%. Prior authorization automation compresses processing time from days to minutes. The American Medical Association reports that AI-driven documentation saves organizations over 15,000 hours annually. These savings come from reducing manual coordination between systems, not from replacing clinical judgment.
Related Resources

Give your healthcare AI agents a persistent workspace
50GB free storage with auto-indexing, semantic search, and structured document extraction. No credit card, no trial expiration. Connect agents via the Fast.io MCP server.